KRAS Inhibitors for NSCLC: Complete Guide to Latest FDA Approvals 2024
Stay updated on the latest FDA approvals for KRAS inhibitors in non-small cell lung cancer (NSCLC), featuring key advancements and treatment options for patients.
Intelligence Snapshot
Executive Summary
Stay updated on the latest FDA approvals for KRAS inhibitors in non-small cell lung cancer (NSCLC), featuring key advancements and treatment options for patients.
Market Impact
| Regulatory | medium |
|---|---|
| Commercial | medium |
| Competitive | low |
| Investment | low |
Loading intelligence…
Loading intelligence…
Loading intelligence…
Loading intelligence…
Executive Scorecard
Heuristic scores · directional, not investment adviceRegulatory catalyst tracker
Track PDUFA dates, approval milestones, and label updates for sotorasib.
Unlock full calendar →Investor brief
Download a one-page summary of regulatory impact and competitive context.
Explore drug hub →Contents11 sections
Medically Reviewed
by Dr. James Morrison, Chief Medical Officer (MD, FACP, FACC)
Reviewed on: March 30, 2026
KRAS Inhibitors for NSCLC: Complete Guide to Latest FDA Approvals 2024
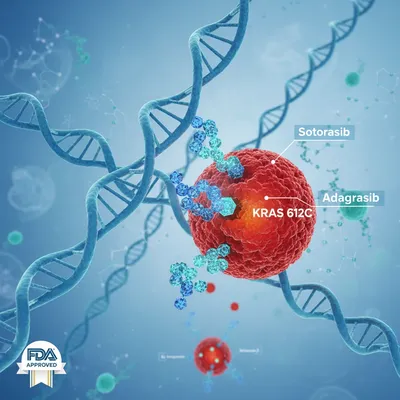
In the evolving landscape of oncology, the approval of KRAS inhibitors heralds a significant advancement in the treatment of non-small cell lung cancer (NSCLC). [Source: U.S. Food and Drug Administration] The U.S. Food and Drug Administration (FDA) has recently approved two pivotal therapies targeting the KRAS G12C mutation: sotorasib (Lumakras) and adagrasib (Krazati). These approvals mark a critical step towards precision medicine, offering hope for patients with this historically challenging mutation.
IntelligenceRegulatory Impact
FDA are the agencies to watch. Regulatory relevance reads medium for oncology, with sotorasib, adagrasib, and lumakras most exposed to upcoming decisions. Teams should track submission types, designations, and guidance shifts that could move approval timelines.
Background: The Significance of KRAS G12C Inhibition
KRAS mutations are prevalent in approximately 25% of NSCLC cases, predominantly the G12C variant. This mutation leads to constitutive activation of the KRAS protein, driving tumor growth and metastasis. Traditional chemotherapy and immunotherapy have shown limited efficacy in this subset of patients, highlighting an urgent need for targeted therapies. The advent of KRAS G12C inhibitors like sotorasib and adagrasib represents a novel therapeutic paradigm, specifically designed to inhibit the mutated KRAS protein and disrupt cancer progression.
IntelligenceCompetitive Intelligence
Competitive pressure is low. Watch which sponsors move first. Benchmark pipeline positioning, differentiation, and partnership scouting against the signals in this story.
Mechanism of Action: How KRAS Inhibitors Work
The mechanism of action for KRAS inhibitors involves selective binding to the inactive form of the KRAS G12C protein, preventing its activation and downstream signaling associated with tumor growth. This selective binding allows for a more targeted approach compared to traditional chemotherapy, minimizing off-target effects. Unlike other targeted therapies that may target earlier components of the signaling pathway, KRAS inhibitors directly address the mutation itself, offering a more efficient blockade of the cancer-promoting signals.
IntelligenceMarket Signals
Commercial pull is medium and investment relevance low. Expect implications for oncology pricing, access, and launch sequencing.
FDA-Approved KRAS Inhibitors
Sotorasib (Lumakras)
Sotorasib was the first KRAS inhibitor approved by the FDA on May 28, 2021, under the accelerated approval pathway for patients with locally advanced or metastatic NSCLC with the KRAS G12C mutation. The approval was based on results from the CodeBreaK 100 trial (NCT03600883), which demonstrated an objective response rate (ORR) of approximately 37% (95% CI, 29%-46%) in this patient population.
The recommended dosing for sotorasib is 960 mg orally once daily. Common side effects include diarrhea, nausea, and fatigue, which were manageable in clinical settings.
Adagrasib (Krazati)
Adagrasib received FDA approval on December 12, 2022, for similar indications in NSCLC patients with the KRAS G12C mutation. This approval was supported by the KRYSTAL-1 study (NCT03785249), which showed an ORR of 43% (95% CI, 34%-53%) among patients treated with adagrasib, highlighting its potential as a robust treatment option.
The approved dosage for adagrasib is 600 mg taken orally twice daily. Adverse effects reported include fatigue, nausea, and increased liver enzymes, which necessitate monitoring during treatment.
IntelligenceStrategic Takeaways
Stay updated on the latest FDA approvals for KRAS inhibitors in non-small cell lung cancer (NSCLC), featuring key advancements and treatment options for patients.
Clinical Trial Data: Efficacy and Safety
The clinical efficacy of KRAS inhibitors is underscored by the results from pivotal trials. In the CodeBreaK 100 trial, the median progression-free survival (PFS) was observed at 6.8 months (95% CI, 5.5-8.6 months), emphasizing the drug's effectiveness in delaying disease progression. In comparison, the KRYSTAL-1 study reported a median PFS of 8.5 months (95% CI, 6.9-10.9 months) for adagrasib.
These trials not only established the efficacy of these agents but also provided critical safety data, with most adverse events being manageable without significant treatment discontinuation.
IntelligenceEvidence Quality
Claims are grounded in the cited primary and secondary sources, with editorial review applied before publication.
Patient Selection and Testing
Accurate patient selection is crucial for the success of KRAS inhibitors. Testing for KRAS mutations is typically performed using next-generation sequencing (NGS) or polymerase chain reaction (PCR) methods to identify the G12C variant. Patient eligibility criteria generally include:
- Histologically confirmed NSCLC
- Presence of KRAS G12C mutation
- Previous treatment with at least one systemic therapy
- No prior treatment with a KRAS inhibitor
Biomarker testing guidelines recommend that all patients with advanced NSCLC should undergo genetic testing to identify actionable mutations, including KRAS G12C, to optimize therapeutic outcomes.
Future Developments: Expanding the KRAS Inhibitor Landscape
As research progresses, several KRAS inhibitors are currently in the pipeline, exploring combination therapies to enhance efficacy and overcome resistance mechanisms. Trials are investigating the synergistic effects of KRAS inhibitors with immune checkpoint inhibitors and chemotherapy. Understanding resistance mechanisms is also a focus, with studies aiming to elucidate how tumors adapt to KRAS-targeted therapies, paving the way for novel treatment strategies.
FAQ Section
What are KRAS inhibitors used for?
KRAS inhibitors are used to treat non-small cell lung cancer (NSCLC) in patients with the KRAS G12C mutation, offering a targeted approach to disrupt tumor growth.
How do sotorasib and adagrasib differ?
Sotorasib and adagrasib are both KRAS G12C inhibitors; however, they differ in their dosing regimens and certain side effect profiles, with clinical trial data supporting their respective efficacy.
What is the significance of KRAS mutation testing?
KRAS mutation testing is critical for identifying eligible patients for KRAS inhibitors, ensuring that those who may benefit from these targeted therapies receive appropriate treatment.
What future developments should we expect for KRAS inhibitors?
Future developments may include new KRAS inhibitors in clinical trials, combination therapies to enhance treatment efficacy, and research into resistance mechanisms to improve patient outcomes.
References
- U.S. Food and Drug Administration. FDA approval. Accessed 2026-03-30.
Related profiles
Related coverage
Continue Exploring
Jump into the entities behind this story.
Ask AI About Oncology
Grounded in NovaPharmaNews intelligence. Pick a prompt to start.
Follow sotorasib developments
FDA oncology alerts and sotorasib pipeline updates, every Monday.
- Evidence strength
- 71/100
- Last verified
- Jun 18, 2026
- AI-assisted review
- Yes
- Editorial review
- Dr. Sarah Chen
Moderate source quality · grounded in cited primary and secondary sources.
This article follows our editorial standards. Report a correction via editorial contact.
About the Author
Continue Your Research

Industry Reports & Whitepapers
- La Negoziazione del Prezzo dei Farmaci Oncologici in Italia — This whitepaper analyzes the market benchmark role in negotiating oncology drug prices in Italy, hig…
- Cytological Specimens in the Molecular Era of Metastatic Melanoma — This whitepaper discusses the role of cytological specimens in diagnosing metastatic melanoma and th…